|
||
|
|
 |
 |
 |
 |
 |
|
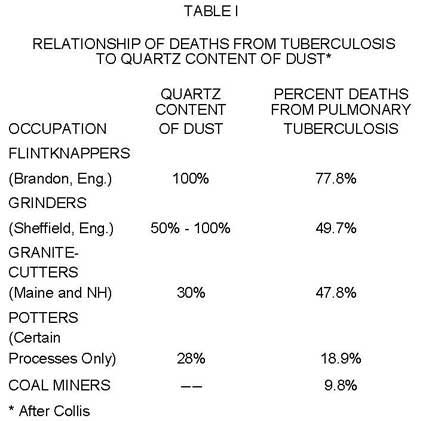
FLlNTKNAPPING AND SILICOSIS By Jeffery Kalin INTRODUCTION: Could early man have been a victim of an industrial disease? I believe this to have been the case. Flintknapping, an activity that dominated more than 99% of the archaeological record of human evolution, turns out to be potentially dangerous to the health of the flintknappers. The process, which involves the breaking of siliceous rocks, produces a fine dust. Repeated inhalation of the free silica particles (Si02) can lead to a pneumonic condition called silicosis or fibrosis. This problem has also been noted by workers in mining, sandblasting, stone carving, road construction and ceramics, where silica is a major cause of pneumonoconiosis or occupational lung disease (Agrecola 1557; Arlidge 1882; Collis 1915; Hunter 1978; Middleton 1930; Oliver 1902 and 1916; Ramazzini 1713; Severo 1980). Prolonged exposure to silica dust particles increases the chance of developing severe silicosis. When microscopic particles are inhaled they pass into the lungs by way of the trachea branching into the two main bronchi. The bronchi, in turn, branch into many tubes which continue to branch repeatedly until each finally terminates in an elongated saccule, the alveolar duct. Branching off this saccule are millions of tiny globular sacs or alveoli. The openings into these sacs are very small, about 5-10 microns. It is in the alveoli that gas exchange takes place with the blood. Our lungs contain approximately 750 million alveoli, which explains why the interior surface area of our lungs is more than fifty times that of the skin of our bodies. Our bodies provide a defense of filters to protect our lungs. The hairs and sinuses of the nose catch the initial dust. The trachea and the larger branches of the bronchial tubes are covered with mucous cells and cilia which protect and clean the lungs of the finer particles. Mucous traps the particles while the beating of the cilia removes dust-laden mucous from the lungs. Problems arise because silicates can break into very small particles, much smaller than 20 microns. These minute flakes enter the deepest part of the lungs, past the mucous and cilia cells in the bronchae and continue until they reach the alveoli, or air transfer sacs. Once these flakes become lodged in the alveoli, they cannot be removed by the lung's natural defense mechanism. The condition becomes more and more serious as the alveoli fill up with razor sharp particles, although the effect is often not felt for many years (usually after 10 to 25 years according to Plunkett, 1976, and 20 to 30 years according to Berkow, 1977). Flintknappers' Exchange 4(2): 1981 HOW SILICOSIS DEVELOPS: Silicosis develops through three recognizable phases (Hunter, 1978; Middleton, 1930). In the beginning the most important symptom is a slight difficulty in .breathing which becomes apparent after exertion, increasing in severity as the condition progresses. A cough may also develop, which is usually "dry", with little mucous. Generally, because (: of the gradualness of the process, individuals feel little immediate effect from the changes taking place in their lungs. Fibrous tissue develops around the dust ladened cells and form:; small round nodules, several millimeters in diameter. These become a permanent part of the lung tissues and are visible by x-ray analysis. Coughing and shortness of breath become noticeable in the next stage. Nodules increase in size and number, occasionally lumping together into conglomerates. Sounds can sometimes be heard in the lungs. A reduced chest expansion, high blood pressure and noticeable effects on working ability are also symptomatic. During the final stage, the dehabilitating effects of the condition are accentuated nodular development, emphysema, and x-ray evidence of growing fibrous masses of tissue. These cause extensive incapacitation of the victim and may ultimately result in death. In addition to the lacerating sharpness of the tiny flakes, a chemical reaction must take place for silicosis to occur (Hunter 1978; Kettle 1932). A soluble substance called silicic acid dissolves off the surface of the stone and polymerizes when it is neutralized by the body tissue. (In polymerization, molecules combine to form long chain compounds of a high molecular weight. This type of reaction is used to make polyethylene or common plastic.) During its creation, polysilicic acid poisons the surrounding tissues. The affected cells appear to be mummified and do not decompose as dead cells in the lungs normally do. What makes flint and quartz particles among the most dangerous of all mineral dusts is the extent to which they dissolve into the blood plasma and the low pH of the acid produced (Hunter 1978). The fibrosis is caused by a poorly understood reaction from the interaction of silica by-products with lung macrophages or defense cells (Cullen 1980). This can be illustrated by comparing flint dust to cement dust which is also high in silicic acid. The high alkaline pH of the limestone in the cement neutralizes the acid and renders it harmless before it reaches the blood plasma and body tissues (Hunter.978). TYPES OF QUARTZ: Some types of quartz dust are more dangerous to inhale than others (Cullen 1980; Stober 1966). There are three major types of silica deposits which constitute the majority of knappable stones: Amorphous, common quartz crystal and cristobalite. Cristobalite is a cubic crystal that forms at high temperatures and is less prevalent than amorphous and common quartz. A fourth type, tridymite, is rare and only encountered in minute traces. The least dangerous, but by no means safe, is the amorphous type which is a quick cooling, crystal free variety. Glass, obsidian and opal are examples of amorphous quartz. Common quartz and quartzite are examples of quartz crystal. Also included in this group are chalcedony, flint, jasper, and chert, all of which are microcrystalline and possess microscopic needle or fiber-like quartz crystals, often arranged in fan-like structures. COMPOSITION OF FLINT: Most flints are composed of 98% silica with 1% to 2% water and minute quantities of impurities which cause color variation. The water appears to be responsible for the exceptional tensile strength of the material (Shepherd 1972). The needle-like, microcrystals of quartz may vary in size and shape from the shorter, stouter type, like those in Irish gray flint, to the long slender crystals found in English black flint. Not all flints are common quartz. Amorphous quartz, cristobalite and tridymite may occur adventitiously also. In Danish flint, which is visually similar to English flint, common quartz was found to range between 4% and 100%. The remainder of its composition was made up of cristobalite, glassy quartz, or a mixture of the two (Shepherd 1972). Traces of tridymite were also found in several samples. Cristobalite has proven to be the most dangerous of the silica dust and workers exposed to cristobalite display a higher incidence of silicosis (Cullen 1980). Cristobalite may also be found in rhyolite, bentinite, obsidian crystal pockets, high fired ceramics, and basalt. DIAGNOSIS OF SILICOSIS: Silicosis is easy to diagnose in its early stages by x-ray and the individual can take appropriate steps to avoid the debilitating and irreversible effects of the advanced stages. An obvious step is to stop exposure to silica dust. Continued exposure will aggravate one's silicosis condition, but there is a difference of opinion as to what happens when a person with silicosis symptoms is no longer exposed to silica dust. In severe cases, it appears the disease does not arrest itself. However, evidence from several studies in England show that when people with early silicosis discontinue their exposure to silica dust, either the disease does not progress, or its development is retarded for a considerable number of years (Middleton 1930; Board of Trade 1945). ADDITIONAL COMPLICATIONS: Curiously, rheumatoid arthritis sufferers show a high rate of incidence of previous exposure to silica dust. This may be explained because silica-ladened white blood cells often re-enter the blood stream from the lungs and thereby transport particles to other lymphatic areas of the body (Cullen 1980). In 1885 Arnold found silica particles included in the liver, the spleen and bone marrow (Arnold 1885). Cuts from knapping may also leave slivers of stone in the body. It also appears that smoking increases the danger of silicosis. Be it today, or in ancient times in the New World, nicotine paralyzes the cilia and prevents the natural cleansing of the bronchial tubes, which results in the bigger flakes being retained. Carving soapstone may cause mesotheleoma (a cancerous lung disease) due to the asbestos fibers in the stone. While silicosis and cancer are found together, there is no proven evidence that silica is a carcinogen (Hunter 1978). In the last year or two, some evidence suggesting silica related cancer has been emerging (Cullen 1980). Ironically, even black lung disease, common among coal miners, is attributed not so much to the coal itself, but to the silica dust present in the coal (Shottenfield 1980). Tuberculosis often accompanies silicosis and the result is a devastating combination. Since it is the most frequently associated complication, tuberculosis plays an important role in silicosis history (Hunter 1978). Capable of infecting other animals (cows, for example) as well as humans, the roots of tuberculosis have been traced back thousands of years in Africa, Asia, Europe, and North and South America. Examples of tubercular disease and deformation have been identified through autopsies of ancient mummies, "deformed bones (Potts disease) and may be seen depicted in examples of prehistoric art work (BrothwellI968; C. Wells 1966; Ritchie 1952). Silicosis has been identified in mummies from Egypt (Harris 1978) and Peru. It is very difficult to differentiate between silicosis and tuberculosis by x-ray alone, and diagnosis should not be made unless additional tests are run. Even in autopsy, the two lung diseases tend to obscure one another, making diagnosis very difficult (Hunter 1978).
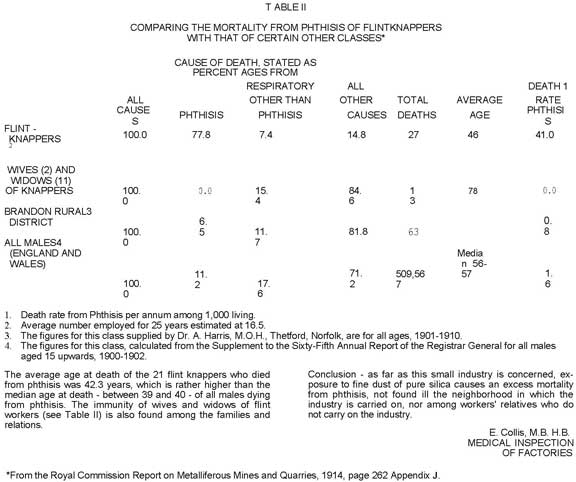
Flintknappers' Exchange 4(2): 1981 There is a direct relationship between the silica content of and industrial dust and workers' deaths from pulmonary tuberculosis. The 1913 study by Dr. E. Collis showed that over three quarters of the flintknappers at Brandon, England died of this problem. He was able to show that workers with silicosis are more prone to contracting tuberculosis and more susceptible to infections from other types of pathogens. Even relatively harmless dusts, when inhaled by a person with mild silicosis, may create a potentially serious pneumonoconiosis condition (Collis 1913). His research concluded that the more different a substance is from those of which the body is naturally composed, the more injurious it is to the body. In light of this information, how can we flintknappers protect ourselves from these dangers? THE DANGERS OF WORKING INDOORS: In 1930, Middleton measured the atmospheric dust produced by two flintknappers working in a shed. His findings showed concentrations as high as 1,313 particles per cubic centimeter, with the majority of the flakes under 1 micron in size. Only 2% of these tiny flakes were over 2 microns. These minute particles easily enter the 20 micron alveolar sacs of the lungs, making silicosis complications from flintknapping understandable. Remembering that a micron is only one thousandth of a millimeter helps you visualize how small these flakes actually are. By definition, particles smaller than 1 micron cease to be called dust and are classified as fumes and those smaller than .3 of a micron are listed as smoke. Imagine the particle counts at a modern indoor knap-in. Errett Callal1an spoke of seeing clouds of dust at the Flintknappers' Exchange 1979 Knap-in at Casper, Wyoming (E. Callahan 1980). During the winter I maintain an indoor workshop in the basement of my house. Since the ventilation is poor, 'I now wear a respirator while working. The Mine Safety Appliances Company in Pittsburg, Pennsylvania makes a mask for dust and fumes that does the job, It is a COMFO 2, custom respirator with a filter cartridge for asbestos-containing dusts, fumes, and mists. While no filter gets everything, the filter meets Mine Safety and Health Administration (MSHA) and National Institute for Occupational Safety and Health (NIOSH) safety requirements. A mask with dual filter cartridges should cost about $20. The cartridges may be' used until they become clogged with dust before changing, but care must be taken not to let the interior of the mask become contaminated with silica dust when it is not being used. To prevent this, I fasten plastic sandwich bags around the cartridges with rubber bands. Be sure to wear your mask while sweeping up debitage. When working indoors, remember it takes over a half an hour for suspended silica dust and fumes to settle (Middleton 1930). An exhaust fan will also prove useful when working indoors. Clothes worn while knapping should be changed, or at least brushed off, after working to avoid tracking dust into living and sleeping areas. Another possibility would be some type of knapping apron to protect clothing from dust. Use of a particle ionizer will also reduce exposure to small particles (electrostatic precipitator). WORKING OUTDOORS: Unless a wind is present, I try to wear a mask while working outdoors, especially when the work is very dusty. When working without a mask, I try to sit so that the wind aids in dust removal. I also try consciously to time my breathing to avoid inhaling the clouds of dust I have just produced, whether from quarrying the stone or finishing a biface with pressure. Fine dust forms whenever the stone is broken. For example, I have found that my platform preparation technique of shearing/abrading tends to produce a lot of visible dust. This can easily be seen when viewed by a strong side light against a dark background. You will notice that while the tiny flakes fall to the ground, a smoke-like powder floats upward, where it is easily inhaled/ Because of this, when I work without a mask, I try to avoid inhaling whenever I see dust while abrading. I hold my breath or slowly exhale, blowing a fine stream of air across my platform. This helps to get the dust away from me so it can be dispersed and removed by air currents. Incidentally, most of the disposable dust masks for sale in hardware and paint stores provide only limited protection and arc inadequate for filtering the suspended silica dust and fumes produced by knapping. HISTORIC: Silicosis is the oldest ~known occupational lung disease (Berkow 1977). Historically, the use of dust masks for flintknapping begins in Brandon, England, where gun-flint knappers wore sponges tied under their noses in an effort to prevent the devastating effects of Phthisis or "knappers rot" (Shepherd 1972). Historically the flintknappers of Brandon, England, still a knapping center, suffered a high mortality rate from silicosis, often with tubercular complications (Collis 1913, 1915). Working mostly in sheds, skilled knappers, who could make three thousand gun flints a day (Webb 1911), were not expected to live much more than forty years (Collis 1913 and 1915; Middleton 1930; Shepherd 1972). The Table (Table II) by Edgar Collis, Medical Inspector for Factories in England, shows the death rate for Brandon Flintknappers. We are most indebted to him for his research. Notice that wives of flintknappers and others not engaged in the profession were not affected by silicosis and had normal life spans. Agrecola (1557) noted that wives of Carpathian miners had as many as seven husbands, due to the high mortality rate among the miners from silicosis. In the "Minutes of Evidence", Collis describes in detail several of the flintknapping families. At the time the study was made, in one family of twenty-six persons (thirteen males and thirteen females), twelve of the males had been flintknappers and ten of them had died. This left two flintknappers and the one 'non-flintknapping male alive, while all thirteen of the women were still alive. In another family of six males, three became flintknappers, Two died leaving one flintknapper and three non-flintknappers alive. In a third family, two of the six males became flintknappers, and only one was still alive to join all four of the non-flintknapping males still living. Collis concluded by saying, "Despite the size of this small industry, there is an excessive mortality problem," In modern Brandon, Mr. Fred Avery, the last of Brandon's flintknappers, said that in an effort to avoid silicosis, he tries to work in a well-ventilated room and limits his knapping to 1-1/2 hours per day. Avery said that because of the historic instances of silicosis and its recorded high mortality, parents in the town discouraged their children from learning to knap (Gould 1980). In France, among the people of the town of Meusenes, the gun-flint industry produced results similar to those at Brandon, England. Chateauneuf said, "By a fate, which seems connected with all that concerns the art of war, this industry slays those who follow it; it kills them before their time; for them there is no old age." When asked the cause of so premature a mortality, doctors and officials gave the same reply-pulmonary phthisis induced by prolonged inhalation of dust generated from working flints" (Collis 1915). Industrialization is probably responsible for these problems among the gun flintknappers, for it is from the continued Flintknappers' Exchange 4(2): 1981
exposure to silica dust that most cases of silicosis occur. If this is so, one would expect that this early industrial disease extended back into the Paleolithic period (Brothwell 1968; Wells 1964; Brothwell and Higgs 1969). Archaeologically; it might be possible to identify it in burials by analysis of the silica content in the dirt in the chest cavity compared to the surrounding soil. Biopsies of lung tissue in mummies could provide valuable data (Harris 1978). By Neolithic times extensive flint mining operations were taking place in northern Europe, and flints were dug and worked by the ton (Bosch 1979). Much of this flint went into making axes, which were often pecked and ground smooth for completion. These processes, if done without water, would produce excessive quantities of dust. Also, if water had been used and then was permitted to dry in the work area, it would allow flint dust to become airborne. Thomas Benson, who in 1713 invented a method for wet grinding flints, states in the patent that the process of dry grinding "proved very destructive to mankind insomuch that a person ever so healthful or strong, working in that business, cannot possibly survive over two years, occasioned by the dust sucked into his body by the air he breathes" (Royal Commission, Vol. 1, Pg. 134). OTHER CAUSES OF SILICOSIS: While industrialized production of stone implements took place in different societies, not all silica workers could be considered flintknappers. Great numbers of craftsmen were exposed to dust as they carved out monumental statues and other constructions. In 1869, Hugo Millers wrote, "The mason is almost always a silent man; the strain on his respiration is too great when he is actively employed to leave the necessary freedom to the organs of speech" (Royal Commission, Vol. 11914). Exposure to volcanic dust after eruption may also cause silicosis. The effects of exposure to high silica ash from Mt. St. Helens should become evident in the coming years (Severo 1980). Throughout time, volcanic eruptions covered different areas of the world with huge amounts of high silica ash. In some places the ash fall was so great that it buried whole cities, such as Pompeii or Thera, or caused entire populations to move, such as the Maya (Trotter 1977). Silicosis also affected workers in the ceramic industry (Arlidgc 1892; Oliver 1902 and 1906). Flint glazes, mixing dry clay and sweeping up the powdery residues are probably the most dangerous activities. Flintknappers' Exchange 4(2): 1981 In Pre-Columbian Mexico and Central America and in the Middle East, large specialized knapping centers developed to serve the elaborate obsidian trade networks that traded blades, bi-faces and ground stone objects. Through chemical-stone analysis it has been possible to trace how specialized craftsmen work daily in special quarry towns to make tools for people hundreds of miles away (Flannery 1976; Dixon 1968). In both these areas of the world, industrial stone knapping still exists today. For example, in the town of Teotehuecan, just north of Mexico City, craftsmen make percussion flaked spear points (projectiles) and carefully carved and polished obsidian objects. These are decorative rather than functional products, manufactured for the tourist market which has carried many of these items as far as Europe, Australia, and Asia (personal observation). Stone tool making on a functional basis can be seen today in northwestern Turkey. Here professional flintknappers make direct percussion blades used in threshing sledges during the wheat harvest. A good knapper can manufacture almost 500 pounds of blades a day if the flint has been quarried beforehand. A village can produce about 500 tons a year. The blades are sold to merchants who distribute them throughout the country (Bordaz 1968). Clearly, in these specialized occupations, workers are exposed to excessive quantities of silica dust and occupational lung disease could result. I am unaware of any medical study that has been done on the flintknappers of Turkey or the obsidian workers of present day Mexico, but these would be prime groups to investigate for signs of pneumonoconiosis. Today, unfortunately, many of us find ourselves in a similar situations as we work daily making lithic artifactual replications and the like. Whether for scientific research, pleasure, or commercial production, we have become industrial craftsmen who subject ourselves to excessive amounts of silica dust and the inherent dangers. The questionnaire which follows is an attempt for all of us to find out more about ourselves and flintknapping. Once the data is compiled, the results will be made available in a future issue of Flintknappers' Exchange. The Brandon history need not repeat itself today. By increasing our understanding and awareness of these potential hazards, we should be able to take appropriate steps to protect ourselves against unnecessary pulmonary damage. SUMMARY: Silicosis is caused by the life-long exposure to and accumulation of free silica dust (Si02) in the lungs. Its degree of severity appears to be directly related to density, length of exposure, particle size and type of quartz. The effects are often not felt until many years after exposure. The best way to prevent silicosis is to minimize the inhalation of suspended silica dust. While knapping, this may be accomplished by working outdoors and by wearing a respirator mask. If you are an avid knapper, a respirator would be an important part of your tool kit. Even if you only wear your mask for the more dusty operations, every little bit helps. When working without a mask, try to time your breathing to avoid inhaling the dust. Changing or brushing off your clothes after knapping may also prove useful. Where possible, water should be used when grinding silicates. It is strongly recommended that knapping not be done indoors or in poorly ventilated areas unless a respirator is worn. The last few issues of Flintknappers' Exchange (Volumes 3:1 and 3:2) showed pictures of indoor flintworking with windows shut. In many ways this simulates a prehistoric mining operation, lots of dust and little ventilation, and may be considered very unhealthy and dangerous. Realizing that health problems can arise from flintknapping is only half the battle. We must each take responsibility for taking precautions and changing old habits, to protect our own lives and the lives of those whom we introduce to the art. By taking the necessary precautions, we will be able to continue knapping to a ripe old age, free from the fear of silicosis. I wish to express my appreciation to Errett Callahan, Mark Cullen and Denise Tratolatis for their generous efforts in making this paper possible. BIBLIOGRAPHY Agrecola, G. 1557 De Re Metallica. Froben Basil Arlidge, J.T. 1892 The Hygiene Diseases and Mortality of Occupations. Percival and Company, London. Arnold, J. 1885 Staubinhalation und Staubmetastase. Berlin, Ger· many. Berkow, R. 1977 The Merck Manual. Merck and Company, Rahway, New Jersey. Board of Trade 1945 Provision of Employment in South Wales for Persons Suspended From Mining Industry 0~1 Account of Silicosis and Pneumonociosis. Board of Trade, His Majesty's Stationary Office, London. Bordaz, J. 1969 "Flint-Flaking'in Turkey." Natural History Magazine,78:73-79. 1971 Tools of the Old and New Stone Age. Natural History Press, Garden City, N.Y. Bosch, P.I. 1979 "A Neolithic Flint Mine." Scientific American, 240(6):126-132. Brothwell, D. 1968 The Skeletal Biology of Earlier Human Populations. Pergamon Press Ltd., London, England. Brothwell, D. and Higgs, E. 1969 Science in Archaeology. Praeger Publishing, Inc. New York, New York. Callahan, E. 1980 Personal Communication. Collis, E. 1913 Annual Report of the Chief Inspector of Factories . 1915 Public Health, Volume 28, pp 252··264. Cullen, M. 1980 Personal Communication. Flintknappers' Exchange 4(2): 1981
|